Adjacent tissue transfer involves rearranging/transferring local areas of the skin along with the underlying subcutaneous tissues to repair a defect. The “defect” repaired may be a traumatic wound/injury or may be a defect left after excision of a lesion/mass. Some examples of adjacent tissue transfer include the following techniques:
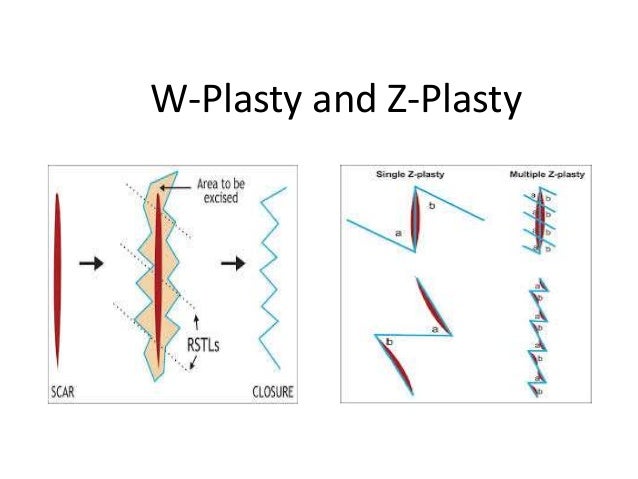
- W-plasty: An adjacent tissue transfer technique where additional incisions in the shape of the letter W are made along the edges of the wound to reduce tension on the edges of the wound and create some laxity in the tissue that allows the wound edges to come together to repair the wound.
- Z-plasty: An adjacent tissue transfer technique where additional incisions are made on either side of a wound creating a shape that resembles the letter Z. These additional incisions create flaps of tissue that are then sutured together to repair the wound.
If you are having trouble picturing what a W-plasty or Z-plasty looks like, check out this link with a great picture of each technique (I’m a visual learner so, for me, pictures are worth a thousand words): W and Z plasty
- V-Y plasty: An adjacent tissue transfer technique where incisions are made in a shape resembling the letter V to create a flap that is then advanced (moved from one position to another) to repair a defect. The final repair which includes a straight line of sutures to repair the area where the flap came from and two additional lines of sutures to sew in the advancement flap in the defect looks like the letter Y which is where this technique “V-Y plasty” gets its name. Again if you are more of a visual learner, here’s a picture showing the “V” portion of the technique in designing the flap and the “Y” portion of the technique in advancing and suturing the flap into place over the defect: V-Y Plasty .
- Rotation flap: An adjacent tissue transfer technique where additional incisions are made to create a flap next to a defect that is then “rotated” over the defect to repair it. Here is a visual for this technique: Rotation Flap
- Random Island Flap: An adjacent tissue transfer technique that involves creation of a flap where the skin is divided all the way around the flap (the incisions completely surround the flap much like water completely surrounds an island which is where this technique gets its name). This island flap receives its blood supply from random non-dominant blood vessels in the subdermal plexus which is where the term “random” island flap comes in. The flap receives blood flow from the donor site where the flap is created and is then moved over or under other tissues to reach the defect needing repair.
- Advancement Flaps: An adjacent tissue transfer technique where incisions are made to create a flap that slides or “advances” forward from its normal location into a defect for repair. Here is a visual for this type of flap: Advancement Flap
There are some other less common techniques that might also fit the definition of adjacent tissue transfer like S-plasty, H-plasty, etc.. As a general rule, though, any technique that involves creating additional incisions to create flaps of tissue that include skin and/or subcutaneous tissues that are then advanced, rotated, or relocated in some manner to repair a defect could meet the definition of adjacent tissue transfer.
Now that we have discussed some common adjacent tissue transfer techniques, let’s take a look at the codes themselves. The first thing we will notice is that there are adjacent tissue transfer codes for specific anatomic sites as long as area requiring the adjacent tissue transfer is not larger than 30 sq cm.
Trunk:
For adjacent tissue transfer of the trunk (e.g., back, chest, abdomen), when the area repaired by adjacent tissue transfer is 30 square centimeters or less, assign one of the following codes:
- CPT 14000: Adjacent tissue transfer or rearrangement, trunk; defect 10 sq cm or less
- CPT 14001: Adjacent tissue transfer or rearrangement, trunk; defect 10.1 sq cm to 30.0 sq cm
Scalp/Arms/Legs:
For adjacent tissue transfer of the scalp, arms, and/or legs when the area repaired by adjacent tissue transfer is 30 square centimeters or less, assign one of the following codes:
- CPT 14020: Adjacent tissue transfer or rearrangement, scalp, arms, and/or legs; defect 10 sq cm or less
- CPT 14021: Adjacent tissue transfer or rearrangement, scalp, arms, and/or legs; defect 10.1 sq cm to 30.0 sq cm
Forehead/Cheeks/Chin/Mouth/Neck/Axillae/Genitalia/Hands/Feet
For adjacent tissue transfer of the forehead, cheeks, chin, mouth, neck, axillae, genitalia, hands, and/or feet when the area repaired by adjacent tissue transfer is 30 square centimeters or less, assign one of the following codes:
- CPT 14040: Adjacent tissue transfer or rearrangement, forehead, cheeks, chin, mouth, neck, axillae, genitalia, hand and/or feet; defect 10 sq cm or less
- CPT 14041: Adjacent tissue transfer or rearrangement, forehead, cheeks, chin, mouth, neck, axillae, genitalia, hand and/or feet; defect 10.1 sq cm to 30.0 sq cm
Eyelids/Nose/Ears/Lips
For adjacent tissue transfer of the eyelids, nose, ears and/or lips, when the area repaired by adjacent tissue transfer is 30 square centimeters or less, assign one of the following codes:
- CPT 14060: Adjacent tissue transfer or rearrangement, eyelids, nose, ears and/or lips; defect 10 sq cm or less
- CPT 14061: Adjacent tissue transfer or rearrangement, eyelids, nose, ears and/or lips; defect 10.1 sq cm to 30.0 sq cm
Once the defect being repaired with adjacent tissue transfer reaches an area of 30.1 sq cm or larger, instead of reporting the codes we have discussed above that are specific for different anatomic sites, we have special codes that are reported for “any area” larger than 30 sq cm.
Any Anatomic Area (Defect larger than 30 sq cm):
When adjacent tissue transfer is performed for a single defect at any anatomic site and the defect is larger than 30 sq cm, report CPT 14301 for the first 60 sq cm and 1 unit of CPT 14302 for each additional 30 sq cm or part thereof.
- CPT 14301: Adjacent tissue transfer or rearrangement, any area; defect 30.1 sq cm to 60 sq cm
- CPT 14302: Adjacent tissue transfer or rearrangement, any area; each additional 30 sq cm, or part thereof
The CPT guidelines have some very specific rules regarding coding adjacent tissue transfer that it is important to understand to ensure proper use of these codes.
Rule #1: If the edges of a wound are “undermined” (lifted up and mobilized) without creating any additional incisions, this is not an adjacent tissue transfer. CPT states that for undermining alone, you should code a complex repair code (CPT codes 13100-13160).
Rule #2: If a traumatic wound is in a shape that “incidentally” results in one of the techniques we just discussed for adjacent tissue transfer (e.g, a W-plasty), this is also not an adjacent tissue transfer. To code adjacent tissue transfer, the surgeon must make incisions and intentionally create the shapes/flaps that meet the definition of adjacent tissue transfer.
Rule #3: Because adjacent tissue transfer can be reported for repair of a defect following excision of a lesion, the excision of a lesion at the same anatomic site as an adjacent tissue transfer is not separately coded. Do not report codes 11400-11446 or 11600-11646 for excision of benign or malignant skin lesions at the site of adjacent tissue transfer.
Rule #4: Adjacent tissue transfer is coded based on the total square centimeters of area repaired with adjacent tissue transfer techniques. When coding adjacent tissue transfer, the term “defect” refers to the primary defect (the area needing repair in the first place) and the secondary defect (any defect created by the effort of designing and mobilizing a flap) together. Add together the total square centimeters of the primary and secondary defect areas to get your total area for repair. Coding tip: Sometimes a surgeon will give you the total area in terms of square centimeters but other times you have to calculate that yourself. If the surgeon provides measurements of the length and width of a wound in centimeters, multiply those measurements together to get your total square centimeters. For example, if a surgeon stated that a traumatic laceration on the arm was 8 cm x 2 cm, and that wound was repaired with a W-plasty, I would multiply 8 x2 to arrive at 16 square centimeters of area for my adjacent tissue transfer code.
Rule #5: If two non-contiguous areas (two areas that are not touching and have distinct margins) are repaired with adjacent tissue transfer and those anatomic areas happen to fall under the same range of CPT codes for a defect that is 30 sq cm or smaller, report separate adjacent tissue transfer codes for each area. For example, if the surgeon performs a rotational flap for an area that is 7 x2 cm on the neck and then an advancement flap for an area that is 3 x4 cm on the foot, you would code 14041 x1 for the adjacent tissue transfer of 14 sq cm on the neck and then 14041 x1 again for the adjacent tissue transfer of 12 sq cm on the foot. On the second line of code with CPT 14041, you would report either modifier 51 or modifier 59 (depending on payer guidelines).
Let’s put this all together with a couple of chart examples.
Example #1: A 55-yr-old patient presents with a traumatic laceration that is 8 x3 cm on the right forearm. After sterile prep and drape, W-plasty relaxing incisions were made along the length of the wound. The edges of the wound then came together nicely allowing us to complete our adjacent tissue transfer over the entire wound surface area. The patient tolerated the procedure well and will be seen in our office in a week for a standard wound check.
Answer Example #1: The bolded portions of the note above are keys to our code selection. We see the wound dimensions are “8 x 3 cm.” We also see the location on the “right forearm.” Next we see the technique used of a “W-plasty” with additional incisions created all along the wound edge to create some laxity in the tissues. Finally, we see that the wound edges comes together and that this adjacent tissue transfer technique of a W-plasty was performed “over the entire wound surface area.” Since the entire wound surface area was repaired with adjacent tissue transfer, we will multiply the length (8 cm) by the width (3 cm) to calculate the total square centimeters of the wound which is 24 sq cm. Since the wound is on the forearm, our code will be CPT 14021.
Example #2: A 66-yr-old patient presents with a very extensive area of melanoma on the back. After sterile prep and drape, the large area of melanoma measuring 10 cm on the lower back was excised down through the subcutaneous fat. Generous wide margins were obtained from the superior, inferior, and lateral margins to ensure complete removal of disease. This left a very extensive defect measuring 20 cm x 5 cm. Next, back cuts were made all along the wound edges, raising rotational flaps that were brought into the defect and sutured to achieve repair. Drains were inserted in the upper portion of the prior defect in the area of deepest dissection. Patient will present to the office in 5 days for a drain removal, wound check, and to discuss final pathology results.
Answer Example #2: Once again, the bolded portions of the note are keys to our code selection. In this case, rather than starting with an open traumatic wound, the surgeon is “excising” melanoma and then repairing a defect created by that excision. As previously discussed, the excision of a malignant skin lesion at the site of adjacent tissue transfer is bundled to the adjacent tissue transfer and should not be reported with a separate code. Here, because the melanoma is excised and then rotational flaps are used for repair in the defect left by the removal of the melanoma, we will not code any additional CPT code for excision of the melanoma.
From there, “back cuts” are made “all along the wound edge.” Back cuts are additional incisions made starting at the wound edge and working outward into the surrounding tissue. These incisions are often used to create flaps along the wound edge that can be brought together for repair. Therefore, the term “back cuts” might be a key word that confirms an adjacent tissue transfer since the required “additional incisions” needed to mobilize adjacent tissue for repair are met by stating that “back cuts” were made. From there, we see the surgeon designing “rotational flaps” that are then “rotated into the defect” and sutured to repair the area. This is an adjacent tissue transfer per CPT guidelines.
While multiple rotational flaps are created, the flaps are all repairing one contiguous large defect of 20 cm x 5 cm left behind after this excision of the melanoma. Since one contiguous defect is repaired, we will code this entire area as “one” for purposes of adjacent tissue transfer. First, we will calculate the total area of repair which is 20 cm x 5 cm or 100 sq cm in total. Since the total area is greater than 30 sq cm, we cannot use codes 14000/14001 even though the adjacent tissue repair is on the back which is part of the trunk. Instead, we need to go to codes 14301/14302 for “any anatomic area” with an adjacent tissue transfer greater than 30 sq cm. We will code CPT 14301 x1 for the first 60 sq cm of repair and then CPT 14302 x2 for the remaining 40 sq cm of repair. Notice, we have 2 units of CPT 14302 since this code is reported for each additional 30 sq cm “or part thereof.” So the first unit of 14302 is coded for an additional 30 sq cm which takes us to 90 sq cm in total when combined with 14301 which captured the first 60 sq cm of repair. We then have 10 sq cm leftover so the second unit of 14302 is for “part of 30 sq cm” (10 sq cm to be exact) which gives us our total repair area of 100 sq cm.
{kind=link}
{kind=link}
{kind=link}
{kind=link}