Category: Article
 Unlock with Patreon
Unlock with PatreonWhat is Included in a Hammertoe Repair (CPT 28285)?
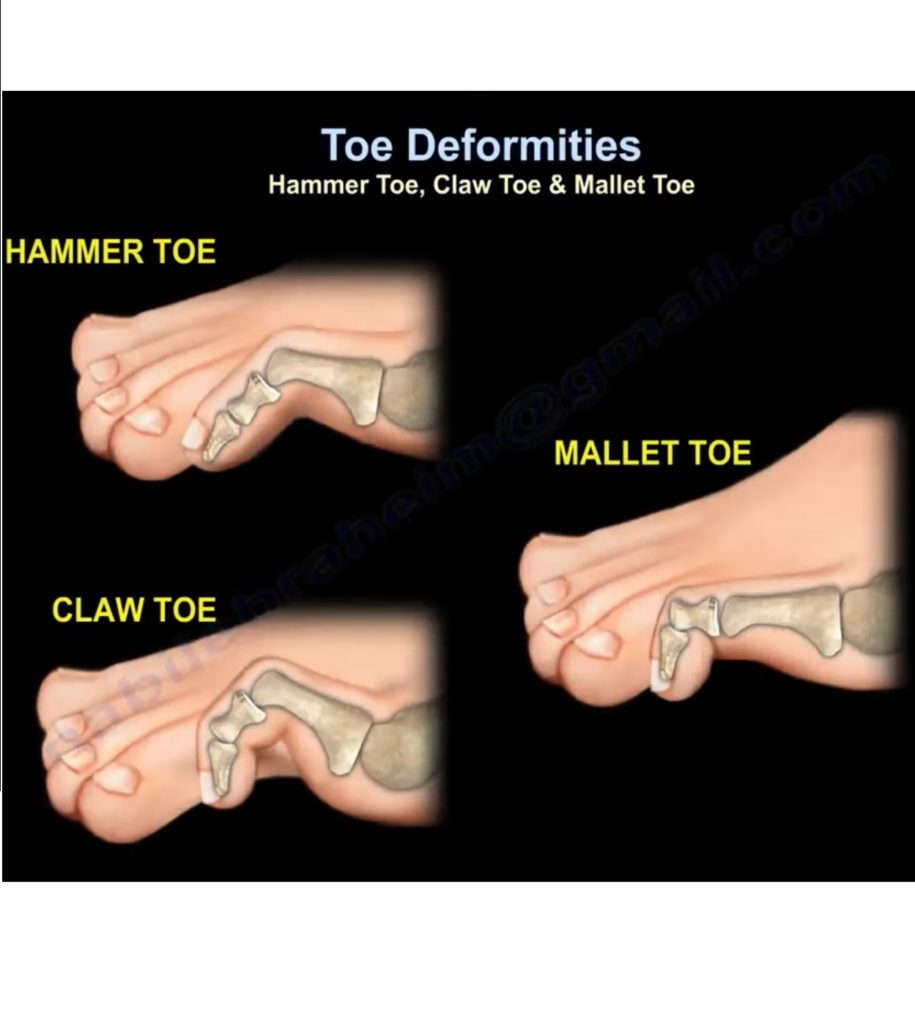
If you work in an orthopedic surgery or podiatry practice, chances are you have coded your fair share of hammertoe repairs. A hammertoe is a deformity where the interphalangeal joint pops up instead of lying flat, giving the toe the shape/appearance of a hammer. For my visual learners, check out this image of a hammertoe: Hammertoe
{kind=link}
While hammertoe repairs are routine procedures for podiatrists, not all operative reports for a hammertoe repair read the same because there are different combinations of surgical procedures that may be required to correct the hammertoe, depending on the severity of the deformity.
So, what exactly is included in CPT 28285 for a hammertoe repair?
Let’s start with the CPT definition of CPT 28285 before looking at some references from CPT Assistant that will further clarify what services are included in this code and what may be separately reported.
CPT 28285: Correction, hammertoe (e.g., interphalangeal fusion, partial or total phalangectomy)
We can see from the CPT description that this code includes removal of part or all of a phalanges (the three small bones that join together to form our toes). It can also include fusion of the interphalangeal joint (the location where two phalanges join). Because our toes have three phalanges, we have two interphalangeal joints. The joint closest to our foot is called the proximal interphalangeal joint (or PIP) while the joint furthest from our foot and closer to the ends of the toes is called the distal interphalangeal joint (or DIP). Fusion of either of these joints is included in CPT 28285.
Excision of the phalanges or fusion of the interphalangeal joints will help the toe to lie flat again and not pop back up after surgery. Notice, though, that in the parentheses of the code description for CPT 28285, we have an “e.g.,” listed before those procedures. This means that excision of the phalanges or interphalangeal fusion are just examples of the types of procedures that may correct a hammertoe.
Here is where CPT Assistant provides more insight on what additional procedures may be included in repairing a hammertoe. The procedures below may be performed as part of a hammertoe repair and should not be coded in addition to CPT 28285 when performed on the same toe:
- Removal of the phalangeal base (CPT 28126)1
- Extensor tendon tenotomy (CPT 28234) 2
- Flexor tendon tenotomy (CPT 28232) 1
- Capsulotomy of the interphalangeal joints (CPT 28272) 1
- Tendon transfer (CPT 28899)4
- K-wire fixation through any joint in the toe undergoing hammertoe repair including the PIP; the DIP; or the metatarsophalangeal (MTP) joint. 1
CPT Assistant also clarifies a key procedure that may be coded separately. A metatarsophalangeal joint capsulotomy (CPT 28270)may be coded in addition to CPT 28285 per CPT Assistant if it is performed to treat a separate deformity (e.g., a contracture of the MTP joint)3. Remember, a hammertoe is a deformity of the interphalangeal joint so deformities of the metatarsophalangeal joint and the treatment of those deformities would be separate and distinct from the hammertoe repair.
Finally, it is also appropriate to code CPT 28285 for repair of a claw toe deformity with extensor tenotomy and flexor tendon transfer. A claw toe deformity is similar to a hammertoe because the interphalangeal joint is bent upwards, but claw toes dig down into the sole of a shoe and can create calluses as a result: Claw Toe Deformity – AAOS. While you may be hesitant to code CPT 28285 for any deformity described with a term other than “hammertoe,” we can code CPT 28285 with confidence since we have a reference from the AMA supporting that coding4.
References:
1CPT Assistant, March 1, 2015, copyright American Medical Association
2CPT Assistant, September 1, 2010, copyright American Medical Association
3CPT Assistant, September 1, 2011, copyright American Medical Association
4CPT Assistant, June 1, 2016, copyright American Medical Association